Point of View: Tuberculosis innovations mean little if they cannot save lives
- McGill University, Canada
- Manipal University, India
- Harvard Medical School, United States
Abstract
The past decade has seen the emergence of new diagnostics and drugs for tuberculosis, a disease that kills over 1.8 million people each year. However, these new tools are yet to reach scale, and access remains a major challenge for patients in low and middle income countries. Urgent action is needed if we are committed to ending the TB epidemic. This means raising the level of ambition, embracing innovation, increasing financial investments, addressing implementation gaps, and ensuring that new technologies reach those who need them to survive. Otherwise, the promise of innovative technologies will never be realized.
https://doi.org/10.7554/eLife.25956.001Main text
As the old saying goes, never bring a knife to a gunfight. And yet, the global tuberculosis (TB) community has been doing exactly that for decades – fighting a protracted battle with antiquated, inefficient tools (Pai et al., 2016), and losing millions of patients in the process.
The most commonly used TB test, sputum smear microscopy, dates back to 1882, the time Robert Koch first demonstrated the bacilli under a microscope. The Bacille Calmette–Guérin (BCG) vaccine, first used in humans in 1921, is still used globally, even though it has been largely ineffective in controlling the TB epidemic. On the treatment front, the TB community had to wait for nearly 50 years for new TB drugs to reach the market.
Lack of good tools has cost us dearly. Last year, the World Health Organization (WHO) declared that the TB epidemic was worse than previously thought, with an estimated 10.4 million new TB cases in 2015 (World Health Organization, 2016a). WHO also estimated that 1.8 million people died from TB in 2015, making TB a bigger killer than HIV and malaria combined.
Thanks to concerted efforts by donors, industry, product development partnerships, and other stakeholders, the past decade has seen the emergence of new diagnostics and drugs for TB. However, these new tools are yet to reach scale, and access remains a major challenge for patients in low and middle income countries (Pai and Schito, 2015; Furin et al., 2016).
Access to new diagnostics
Several new TB diagnostics have emerged on the market and many have also been policy-endorsed by WHO and other agencies (Pai and Schito, 2015). These new diagnostics include Xpert® MTB/RIF (Cepheid Inc, Sunnyvale, California) (World Health Organization, 2013a), line probe assays (World Health Organization, 2016b), urine lipoarabinomannan antigen detection test (World Health Organization, 2015a), liquid cultures (World Health Organization, 2007), and interferon-gamma release assays (World Health Organization, 2014a).
Although it is widely acknowledged that rapid, accurate diagnosis is critical for timely initiation of anti-TB treatment, many people with TB (or symptoms of TB) struggle to access an adequate initial diagnosis. This is underscored by the fact that an estimated 41% of the 10.4 million new cases globally are either undiagnosed or not reported (World Health Organization, 2016a). These “missing” 4.3 million people with TB contribute to ongoing TB transmission, including the transmission of multidrug-resistant TB (MDR-TB).
Even if diagnosed with TB, access to universal drug-susceptibility testing is far from reality for most patients in high burden settings. Nearly 75% of the 480,000 cases of MDR-TB are either not detected or not reported (World Health Organization, 2016a). Even among previously treated patients at risk of drug-resistance and mortality, nearly 40% are not tested for drug resistance.
Cumulatively, since the launch of the Xpert MTB/RIF assay in 2010, over 6,500 GeneXpert machines and 23 million Xpert MTB/RIF cartridges had been procured in the public sector in 130 of the 145 countries eligible for concessional pricing, as of 31 December 2016 (World Health Organization, 2017a; Figure 1). While this trend is promising, the volume of Xpert MTB/RIF testing remains a small proportion of all TB tests conducted in high burden countries. It is estimated that over 77 million sputum smears are performed annually in 22 of the highest TB burden countries, including follow-up tests (Kik et al., 2014). With the notable exception of South Africa, which has rolled-out Xpert MTB/RIF on a national scale and accounts for almost 50% of global Xpert MTB/RIF volumes, other countries are still reliant on insensitive smears (FIND et al., 2015). This is reflected in the ratio of smear volumes to the number of Xpert MTB/RIF cartridges procured. In 2014, the ratio in South Africa was 1.6 – significantly lower than most other high burden countries, where approximately 40–70 smears were performed for each Xpert MTB/RIF test (Qin et al., 2015). Although the ratio has become more favorable to Xpert MTB/RIF in 2015, smears still dominate the TB testing landscape in high burden countries (Danielle Cazabon, personal communication).
Figure 1
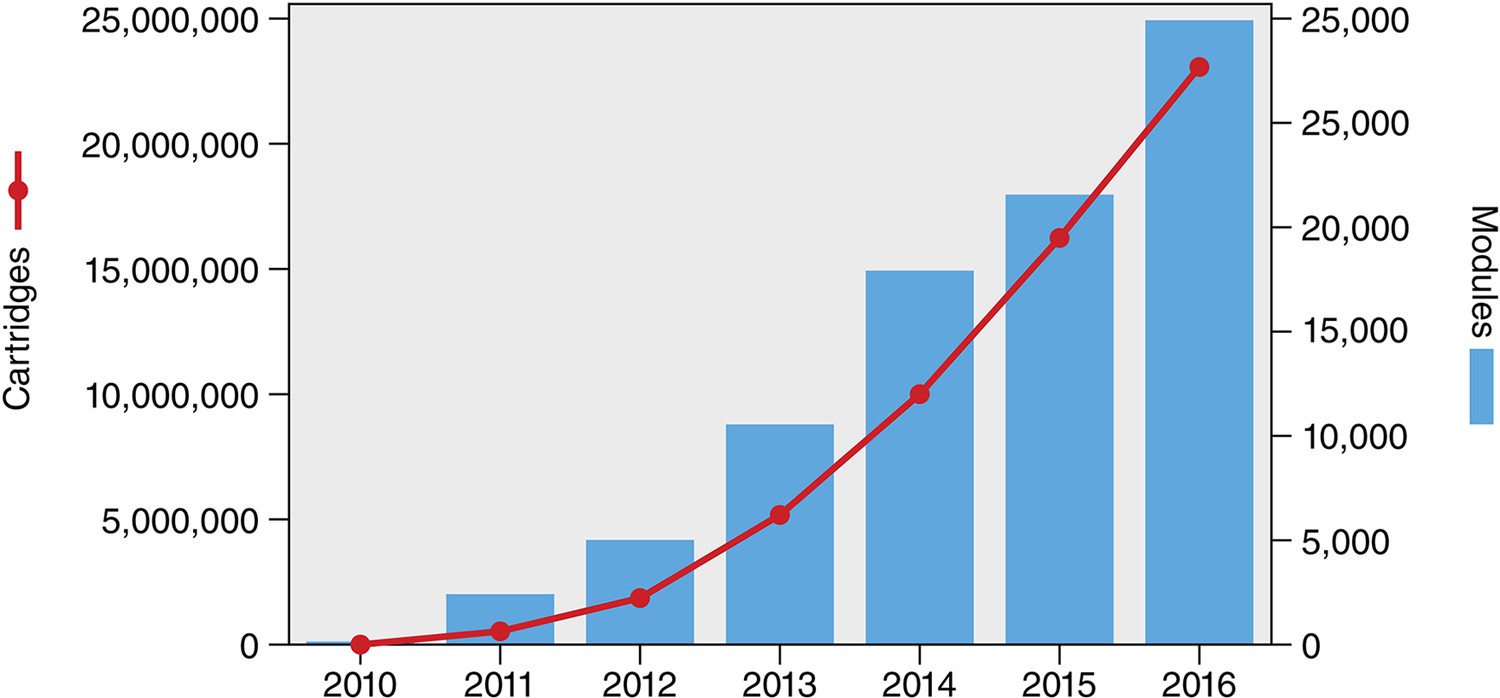
Cumulative number of GeneXpert instrument modules and Xpert MTB/RIF cartridges procured under concessional pricing since 2010.
As of 31 December 2016, a total of 6,659 GeneXpert instruments (comprising 29,865 modules) and 23,140,350 Xpert MTB/RIF cartridges had been procured in the public sector in 130 of the 145 countries eligible for concessional pricing. Source: Cepheid & WHO (World Health Organization, 2017a).
From a policy perspective, only eight countries have made Xpert MTB/RIF the initial diagnostic test for all people suspected of having TB, despite the high accuracy of the test and its ability to rapidly detect drug resistance (Albert et al., 2016). Even when the technology is available, access is limited to patients. A recent large, international study of Xpert MTB/RIF access and utilization in 18 countries found that the majority of sites had access to Xpert MTB/RIF, but only 4% of TB/HIV co-infected patients were actually tested using Xpert MTB/RIF (Clouse et al., 2017). Lack of diagnostics with high sensitivity, and inadequate access to drug-susceptibility testing forces patients to make multiple visits and spend a lot of money, and increases morbidity (Chavan, 2017).
Children are an especially vulnerable population when it comes to TB and MDR-TB. Although tools like Xpert have been endorsed for use in children (World Health Organization, 2013a), and Xpert has been shown to greatly improve the detection of MDR-TB in children (Raizada et al., 2014), access remains a concern in this subgroup.
Why are new TB diagnostics not reaching the patients who need it the most? As reviewed by Albert and colleagues (Albert et al., 2016), the roll-out of Xpert MTB/RIF has highlighted major implementation gaps that have constrained scale-up of this technology and limited its impact on patient outcomes. The roll-out has been hampered by high costs for cash-starved national TB control programs in high-burden countries. It is not just the cost of testing, but also the cost of treating MDR-TB, since Xpert MTB/RIF invariably identifies more patients with drug-resistance than conventional testing.
Another barrier for scale-up of Xpert MTB/RIF has been a lack of a complete diagnostic package for TB that includes comprehensive training, quality assurance, implementation plans, and maintenance support (Albert et al., 2016). Also, pragmatic trials have shown that the clinical impact of Xpert has been blunted by weak health systems, resulting in prolonged time to diagnosis and treatment, compounded by empirical therapy by healthcare providers (Theron et al., 2014; Durovni et al., 2014; Churchyard et al., 2015).
In India, for example, an average TB patient is diagnosed after a delay of nearly two months and after seeing three providers (Sreeramareddy et al., 2014), and diagnosis is a major gap in the cascade of care in the public sector (Subbaraman et al., 2016) and the private sector (Das et al., 2015). In South Africa, even though Xpert MTB/RIF and line probe assays are freely available in centralized laboratories, studies show long delays between sample collection and initiation of TB treatment (Hanrahan et al., 2012; Naidoo et al., 2014), and missed opportunities to deploy tests that are available (Chihota et al., 2015).
In many countries the private sector plays a dominant role in care provision, yet this sector has been excluded from concessional Xpert MTB/RIF pricing, resulting in high costs for patients who pay an average price of nearly USD 70 for the test (Puri et al., 2016). In addition, quality of TB care, especially diagnosis, is a concern in the private sector (Das et al., 2015). Addressing this requires a comprehensive private sector engagement strategy that includes patient-centric quality care as a centerpiece (Cazabon et al., 2017).
In many countries, TB control receives limited domestic funding, and many low-income countries are heavily reliant on external donor funding (Floyd et al., 2013). India is a case in point. Despite having the largest number of TB patients in the world, the country’s governmental expenditure on health is one of the lowest in the world at 1.4% of GDP (The Lancet, 2017). This under-investment is reflected in India’s Revised National Tuberculosis Control Program (RNTCP), which has struggled to receive budgets necessary to tackle the world’s biggest TB epidemic (Pai et al., 2017). This, in turn, has made India rely heavily on old tools such as smear microscopy. Although over 600 GeneXpert systems are now available in the Indian public sector, and have been shown to dramatically increase the MDR-TB case detection rates (Sachdeva et al., 2015), the country has restricted the use of this technology primarily to individuals at risk of MDR-TB, persons with TB/HIV co-infection, and children. This might improve with India’s new, ambitious plan to eliminate TB by 2025, although it is unclear whether India’s TB control budget will match the ambition (Pai et al., 2017).
Access to new drugs
Even if access to new diagnostics was to be dramatically improved, patients still need adequate access to drugs. The past five years have been a period of great potential with the introduction of two new therapeutic agents for the treatment of MDR-TB: delamanid (Otsuka Pharmaceutical Co, Tokyo, Japan) and bedaquiline (Janssen Therapeutics, NJ, USA) (Gler et al., 2012; Diacon et al., 2014; Field et al., 2012). Both drugs have been conditionally approved by stringent regulatory authorities and recommended by the WHO for the treatment of MDR-TB in situations in which there is resistance or intolerance to the other second-line agents or a high risk of treatment failure (World Health Organization, 2013b; World Health Organization, 2014b).
Although there was initial excitement about the availability of these new drugs, because they were approved using phase IIB data, their use was recommended in a cautious way (World Health Organization, 2013b; World Health Organization, 2014b, World Health Organization, 2017b). Since then, global introduction has not kept pace with the dire need for these drugs, especially for patients with drug-resistant disease who endure prolonged, toxic therapies with poor outcomes (Lessem et al., 2015). Complicating this have been the long delays seen in starting pivotal late-stage clinical trials for MDR-TB (RESIST TB, 2017).
A conservative estimate is that one-third of newly diagnosed patients with rifampicin-resistance will have an indication for a new drug during the treatment for MDR-TB, although some studies suggest that as many as two-thirds of patients would benefit from the new drugs (Bonnet et al., 2016). This means that there are between 200,000 and 400,000 persons in need of the novel medications each year. Even a more conservative estimate, based on a third of the total number of persons actually started on MDR-TB treatment each year, reveals a major access gap among the 41,667 patients who urgently need these medications each year.
Currently, just over 8,000 patients have ever received either bedaquiline or delamanid for the treatment of MDR-TB under program conditions (DR-TB STAT, 2017). Recent optimistic reports about new drug uptake released by the WHO – which state there are 70 countries using bedaquiline and 39 using delamanid – are somewhat misleading in that they count any country that has treated a single patient with a new drug, even under compassionate use conditions (World Health Organization, 2016a).
There is tension between wanting to “protect the new drugs” as opposed to protecting the lives of patients
Program use data shows that as of March 1, 2017 there were 8,195 persons who have ever taken bedaquiline and 496 who have ever taken delamanid under program conditions (DR-TB STAT, 2017; Figure 2). Of note, 60% of global bedaquiline use is from South Africa (DR-TB STAT, 2017). So, most countries are either not using the new drugs or are focused only on small pilot projects. One example of this is in the Pan-American Health Organization (PAHO) region of the world, where it is estimated that there are more than 7,000 patients in need of either bedaquiline or delamanid, but fewer than 100 individuals who have received either of these medications.
Figure 2
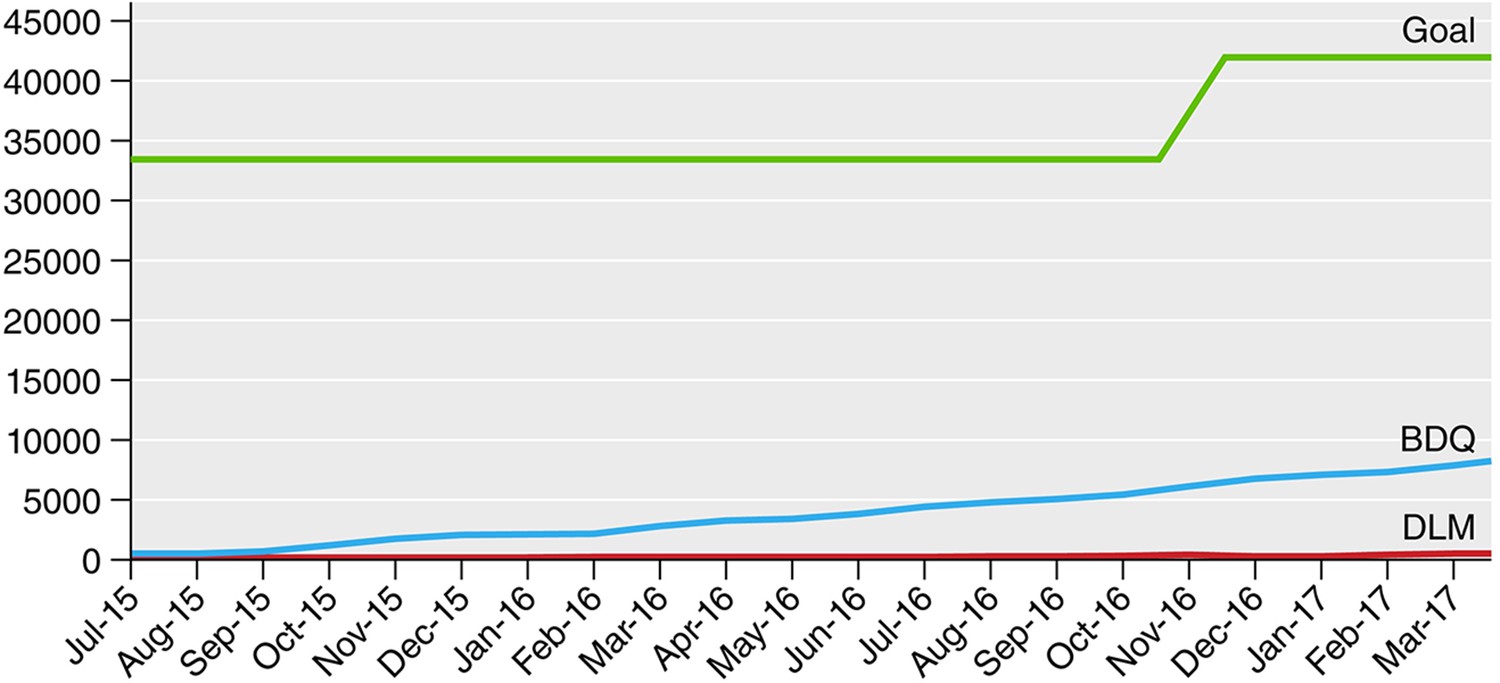
Progress in bedaquiline (BDQ) and delamanid (DLM) global uptake by month compared with estimated need (goal).
Source: DR-TB STAT (DR-TB STAT, 2017).
There are several barriers for wider use of bedaquiline and delamanid (Furin et al., 2016). Some of these are related to costs and registration. Although there is a bedaquiline donation program that allows Global Fund eligible countries to obtain bedaquiline free of charge, countries who are not eligible for this donation often pay a high price via a tiered pricing structure, with middle-income countries paying USD 3,000 for a six-month course of the drug, and high income countries paying as much as USD 26,000 for the six-month course – costs that are almost impossible to bear for poorly funded TB programs (Gotham et al., 2017). Some countries, however, have recognized that the cost of purchasing bedaquiline is lower than the cost to health systems of the ongoing spread of MDR-TB, as seen in the successful South African program. South Africa has to purchase its own bedaquiline yet it accounts for more than 60% of the global use (Ndjeka, 2016).
Delamanid is available for purchase at USD 1,700 for Global Fund eligible countries, but the costs in non-Global Fund eligible countries are excessive and may be as much as Euro 30,000 (approximately USD 32,000) in some settings (Gotham et al., 2017). While bedaquiline has been registered in a range of countries – including the high burden countries of South Africa and India – delamanid only has regulatory approval in four regions: European Union, Japan, South Korea, and Macau. None of these areas have a high burden of MDR-TB, and delamanid is still not registered in most of the countries where clinical trials were done.
Other important country-level barriers seem to be driving the slow uptake of new drugs on the part of national TB programs, regulatory agencies, and clinical providers. Some of these barriers are based in excessive concern about potential side effects, a concern that needs to be balanced with the high mortality rate in persons with poorly treated MDR-TB and the high rate of serious adverse events that occur using the existing medications (Ahuja et al., 2012). There is tension between wanting to “protect the new drugs” as opposed to protecting the lives of patients, with the drugs being restricted in order to purportedly preserve their efficacy. This was the situation in a recent court case where a young woman and her family sued the Indian government to provide her with access to bedaquiline – a case they won – but the government argued that doing so would risk the development of bedaquiline resistance (Kirby, 2017).
There has been almost no involvement of the private sector in the use of new drugs, even in private sector tertiary care facilities that have a proven track record in the successful management of MDR-TB (Udwadia et al., 2017). There are also complicated pharmacovigilance requirements for new drugs (World Health Organization, 2015b) that have delayed their use in some settings (Furin et al., 2016). And most countries feel compelled to follow the interim WHO guidance to the letter on the use of these medications, and guidelines can lag behind the most relevant safety and efficacy data. Given the rapid accumulation of data on the safety and efficacy of these drugs, rigid adherence to interim policies can delay access to life-saving drugs for patients. It should be noted, however, that most countries are unable to implement new drugs even following these restrictive recommendations.
Children are especially vulnerable to TB and MDR-TB and they have been largely overlooked when it comes to access to the new drugs, even though delamanid was recommended by the WHO for children as young as six years of age in 2016. Such exclusion is often a result of a desire to “protect” children from the unknown adverse effects of novel agents, a practice that is especially concerning given the well-known toxicity of the injectable agents (Weld et al., 2017). Not only is there a need to include children earlier in the clinical trials of novel agents (Nachman et al., 2015), but there is also a need to develop child-friendly formulations of the medications (Furin et al., 2015), something that is being pursued with both bedaquiline and delamanid. Other populations vulnerable to exclusion include pregnant women and persons with extrapulmonary TB. Thus, countries should make plans for off-label use of new drugs in these individuals, should the benefits outweigh the risks.
Silver linings and potential solutions
Amidst the disappointingly slow pace of new tool uptake, there are some positive examples and potential solutions. South Africa has been exceptional in scaling-up both Xpert MTB/RIF and bedaquiline, due in large part to a forward-thinking National TB Program and Department of Health, backed by an ambitious Health Minister, and supported by academic and non-governmental organization partners (Ndjeka et al., 2015). Other countries too have had success introducing bedaquiline, especially when they prioritized patient needs, were flexible with their innovations, and partnered with other supporting groups (Guglielmetti et al., 2017). Also, the early success of tools like Xpert MTB/RIF and bedaquiline have renewed industry engagement in TB R&D, pushed countries to develop systems for conducting field trials for policy changes, and revitalized front-line health workers and civil society (Pai and Schito, 2015; Furin et al., 2017). It is also wonderful to see countries develop more ambitious plans for TB elimination, with India being a prominent, recent example (Central TB Division, 2017).
It is wonderful to see countries develop more ambitious plans for TB elimination, with India being a prominent recent example
Many of the barriers to optimal use of novel diagnostic and therapeutic strategies can be readily surmounted with bold ambitions that are followed up with concrete implementation. With regards to new diagnostics, we need a comprehensive approach to their implementation (Albert et al., 2016), including increased engagement of patients, civil society, and policy makers; demand creation for new tools among diverse stakeholders; broader health systems strengthening in preparation for new tools; increased advocacy for TB financing; and market-based approaches to address both demand and supply side barriers (Engel et al., 2016). These solutions are particularly relevant as WHO recently endorsed the use of Xpert MTB/RIF Ultra, a more sensitive assay than the current Xpert MTB/RIF cartridge (World Health Organization, 2017c), and point-of-care molecular diagnostics (e.g. GeneXpert Omni) are becoming a reality.
When it comes to the novel agents, while there are indeed limited data on their use in large populations, this should always be considered in the context of currently recommended treatment regimens, which are based on expert opinion and observational data, are associated with poor treatment outcomes, and are associated with an unacceptable safety profile that has been well documented. When viewed through this lens, the introduction of new therapeutic options can only be seen as a welcome event. The WHO must take this into account, and release unified MDR-TB guidelines that are consistent in their use of recommendations based on observational and programmatic data. There has now been sufficient experience in the successful introduction of novel agents for MDR-TB, and the programs and providers responsible for this success should be leading the global rollout of these drugs. Finally, urgent patient needs must be prioritized, with the organizations and agencies failing to address these needs being held accountable for delayed or denied access. After all, “protecting human rights, ethics and equity” is one of the four key principles of the WHO End TB Strategy (World Health Organization, 2017d).
Conclusions
New diagnostic and treatment options have been sought for decades in the field of TB and MDR-TB, and new tools have been successfully introduced. But we have learnt the hard way that availability does not necessarily result in widespread access. Considerable effort is required to make sure new tools are made accessible to the persons who need them most. This has not happened as quickly as desired with tools such as Xpert MTB/RIF, bedaquiline, and delamanid, and the result is that tens of thousands of TB patients around the world suffer needlessly from late or misdiagnosis, ineffective treatment, or intolerable side effects. The mere fact that 1.8 million people die of a potentially curable infection each year is the surest indication that they are not getting the quality care they deserve.
Urgent action is needed if we are committed to ending TB in a mere 13 years. This means embracing innovation, increasing financial investments in TB control, addressing implementation gaps, and making sure that new technologies are available in the service of those who are trying to survive. More importantly, the global TB community needs to learn from the HIV/AIDS experience, and raise its level of ambition. This means a change in the mindset, to not settle for less.
References
-
Identification of patients who could benefit from bedaquiline or delamanid: a multisite MDR-TB cohort studyThe International Journal of Tuberculosis and Lung Disease 20:177–186.https://doi.org/10.5588/ijtld.15.0962
-
Quality of Tuberculosis care in high burden countries: the urgent need to address gaps in the care cascadeInternational Journal of Infectious Diseases 56:111–116.https://doi.org/10.1016/j.ijid.2016.10.016
-
ReportNational Strategic Plan for Tuberculosis Elimination 2017–2025 (Draft)New Delhi: Ministry of Health & Family Welfare. Government of India.
-
Use of standardised patients to assess quality of tuberculosis care: a pilot, cross-sectional studyThe Lancet Infectious Diseases 15:1305–1313.https://doi.org/10.1016/S1473-3099(15)00077-8
-
Multidrug-resistant tuberculosis and culture conversion with bedaquilineNew England Journal of Medicine 371:723–732.https://doi.org/10.1056/NEJMoa1313865
-
New treatment options for multidrug-resistant tuberculosisTherapeutic Advances in Respiratory Disease 6:255–268.https://doi.org/10.1177/1753465812452193
-
TB Diagnostics Market in Select High-Burden Countries: Current Market and Future Opportunities For Novel DiagnosticsTB Diagnostics Market in Select High-Burden Countries: Current Market and Future Opportunities For Novel Diagnostics, https://www.mcgill.ca/tb/files/tb/tb_diagnostics_market_in_select_high-burden_countries_current_market_and_future_opportunities_for_novel_diagnostics.pdf.
-
Combating drug-resistant tuberculosis: the unexpected benefits of bedaquilineThe International Journal of Tuberculosis and Lung Disease 21:4–5.https://doi.org/10.5588/ijtld.16.0768
-
A bitter pill to swallow: the need for better medications for drug-resistant tuberculosis in childrenThe International Journal of Tuberculosis and Lung Disease 19 Suppl 1:55–60.https://doi.org/10.5588/ijtld.15.0380
-
Delamanid for multidrug-resistant pulmonary tuberculosisNew England Journal of Medicine 366:2151–2160.https://doi.org/10.1056/NEJMoa1112433
-
Estimated generic prices for novel treatments for drug-resistant tuberculosisJournal of Antimicrobial Chemotherapy 72:dkw522.https://doi.org/10.1093/jac/dkw522
-
Examples of bedaquiline introduction for the management of multidrug-resistant tuberculosis in five countriesThe International Journal of Tuberculosis and Lung Disease 21:167–174.https://doi.org/10.5588/ijtld.16.0493
-
Replacing smear microscopy for the diagnosis of tuberculosis: what is the market potential?European Respiratory Journal 43:1793–1796.https://doi.org/10.1183/09031936.00217313
-
Landmark legal ruling sees Indian girl prescribed bedaquiline for XDR-TBThe Lancet Respiratory Medicine 5:249.https://doi.org/10.1016/S2213-2600(17)30042-5
-
Access to new medications for the treatment of drug-resistant tuberculosis: patient, provider and community perspectivesInternational Journal of Infectious Diseases 32:56–60.https://doi.org/10.1016/j.ijid.2014.12.012
-
Towards early inclusion of children in tuberculosis drugs trials: a consensus statementThe Lancet Infectious Diseases 15:711–720.https://doi.org/10.1016/S1473-3099(15)00007-9
-
Treatment of drug-resistant tuberculosis with bedaquiline in a high HIV prevalence setting: an interim cohort analysisThe International Journal of Tuberculosis and Lung Disease 19:979–985.https://doi.org/10.5588/ijtld.14.0944
-
ConferenceIncorporation of bedaquiline in the South African National TB program2016 Conference on Retroviruses and Opportunistic Infections.
-
Tuberculosis diagnostics in 2015: landscape, priorities, needs, and prospectsJournal of Infectious Diseases 211 Suppl 2:S21–S28.https://doi.org/10.1093/infdis/jiu803
-
How is Xpert MTB/RIF being implemented in 22 high tuberculosis burden countries?European Respiratory Journal 45:549–554.https://doi.org/10.1183/09031936.00147714
-
WebsiteResearch excellence to stop TB resistance. Clinical trials progress reportResist-TB. Accessed 2017.
-
Delays in diagnosis and treatment of pulmonary tuberculosis in India: a systematic reviewThe International Journal of Tuberculosis and Lung Disease 18:255–266.https://doi.org/10.5588/ijtld.13.0585
-
Compassionate use of bedaquiline in highly drug-resistant tuberculosis patients in Mumbai, IndiaEuropean Respiratory Journal 49:1601699.https://doi.org/10.1183/13993003.01699-2016
-
The time has come: the case for injectable-sparing regimens in children with multidrug-resistant tuberculosisThe Lancet. Respiratory Medicine 5:245–246.https://doi.org/10.1016/S2213-2600(17)30078-4
-
ReportPolicy Update: Automated Real-Time Nucleic Acid Amplification Technology for Rapid and Simultaneous Detection of Tuberculosis and Rifampicin Resistance: Xpert MTB/RIF System for the Diagnosis of Pulmonary and Extrapulmonary TB in Adults and ChildrenGeneva, Switzerland: World Health Organization.
-
ReportThe Use of Bedaquiline in the Treatment of Multidrug-Resistant Tuberculosis: Interim Policy GuidanceGeneva, Switzerland: World Health Organization.
-
ReportGuidelines on the Management of Latent Tuberculosis Infection. WHO/HTM/TB/2015.01Geneva, Switzerland: World Health Organization.
-
ReportThe Use of Delamanid in the Treatment of Multidrug-Resistant Tuberculosis: Interim Policy GuidanceGeneva, Switzerland: World Health Organization.
-
ReportThe Use of Lateral Flow Urine Lipoarabinomannan Assay (LF-LAM) for the Diagnosis and Screening of Active Tuberculosis in People Living with HIV. Policy UpdateGeneva, Switzerland: World Health Organization.
-
ReportActive Tuberculosis Drug Safety Monitoring and Management (ADSM): A Framework for Implementation. WHO/HTM/TB/2015.28Geneva, Switzerland: World Health Organization.
-
ReportGlobal Tuberculosis Report 2016Geneva, Switzerland: World Heath Organization.
-
ReportThe Use of Molecular Line Probe Assays for the Detection of Resistance to Second-Line Anti-Tuberculosis Drugs. Policy GuidanceGeneva, Switzerland: World Health Organization.
-
ReportReport of the Guideline Development Group Meeting on the Use of Bedaquiline in the Treatment of Multidrug-Resistant Tuberculosis, a Review of Available Evidence (2016)Geneva, Switzerland: World Health Organization.
-
ReportWHO Meeting Report of a Technical Expert Consultation: Non-Inferiority Analysis of Xpert MTB/RIF Ultra Compared to Xpert MTB/RIFGeneva, Switzerland: World Health Organization.
Decision letter
-
Emma PewseyReviewing Editor; eLife, United Kingdom
In the interests of transparency, eLife includes the editorial decision letter and accompanying author responses. A lightly edited version of the letter sent to the authors after peer review is shown, indicating the most substantive concerns; minor comments are not usually included.
Thank you for submitting your article "Tuberculosis innovations mean little, if they cannot save lives" for consideration by eLife. Your article has been reviewed by 3 peer reviewers. The following individuals involved in review of your submission have agreed to reveal their identity: Jane Coyne (Reviewer #3).
I've copied the reviews below. In general, the reviewers were enthusiastic about the article, but they each have a number of points they would like you to address in a revised version of your article. Please try to address all these points in your revised version, or explain in the cover letter accompanying your resubmission why you did not feel it was essential to do so.
Reviewer #1:
1) Although there is nothing wrong in publishing this article as such, considering the authors' expertise, vast experience in the field of TB and other infectious diseases, they should also include few constructive suggestions on the above aspects than being generic.
2) Also, often time researchers ignore the necessity to concentrate more on the follow-up of TB cases started on treatment, and bacteriological confirmation at various time points to ensure the completion of treatment and disease free status. There is no diagnostic test available at present to differentiate dead and viable bacteria. Even the famous Bangladesh study relied only on vital staining techniques such as FDA/ EB based microscopy to prove that the MDR cases are not secreting non-viable bacilli. Considering this need, the authors must urge the scientific community to concentrate on this aspect as well.
3) People generally tend to ignore paediatric and extra-pulmonary TB cases due to diagnostic constraints. Although XPert does wonders in the early detection of such cases, access becomes difficult and also specimen collection, which requires additional provision including hospitalization, negates the optimal utility of XPert. With any new technique when the sensitivity gets enhanced, the danger of quality being compromised lingers on. To overcome this, the necessity to establish quality assurance in public and private care should be included.
4) Likewise, the easy access and availability of drugs in suitable formulations for paediatric TB cases should be advocated. This applies more so for newer drugs.
5) The upcoming improved version of Xpert such as XPert Ultra, Omni and other methods such as TB LAMP, True NAT etc may also be mentioned to show that some hope is on the horizon.
6) Finally TB control should be inclusive and we are all aware that involving private care remains mostly on paper now for various reasons. Until the respective governments give their commitment by way of legislation or decree, we will be rendering mostly lip service and any amount of writing may not solve the problem. This may be advocated in the UN Assembly as and when they hold a special session on TB Control. Can this be considered by the authors and also other points submitted.
Reviewer #2:
1) The authors omit to mention that Bdq and Dlm are not fully approved by any SRA but got either accelerated or conditional approval by FDA or EMA after their phase IIb. This justifies the pharmacovigilance requirements and partly explains the reluctance of some countries to use these drugs.
2) The paper fails to recognize and describe the major obstacles that lie at country level (regulatory authorities, NTPs, or reluctance from clinicians): India which is eligible to GF is limiting access to Bdq to 6 centers of excellence for a country of 1.3 billion inhabitants; Peru, despite registration and free access to Bdq has only enrolled 71 patients, Philippines 51, etc.
3) Presenting the cost as a major obstacle to access is somehow contradicted (or at least tempered) by the facts: there is very little uptake of Bdq by most GF eligible countries for which Bdq is free (numerous examples: Peru, Kyrgyzstan, Bangladesh, India, etc.) when South Africa (which pays Bdq at 900 USD per treatment because of internal procurement mechanism) is far ahead with over 4,000 treatments.
4) There is no doubt that the WHO recommendations on new drugs should be revised, however most countries are far from even reaching the current WHO recommended indications. One could quite easily make estimates showing that following these recommendations "to the letter", as the authors say, would rather result in a much greater uptake than what is actually observed.
5) Minor comments
-77 million sputum smears is a bit misleading as it includes the follow-up smears
- Presenting the costs of the new drugs in high income countries is not relevant to the scope of the paper
- I would suggest referencing the WHO guidelines for Xpert, LPA, LAM, etc.
- Bonnet et al. found that 2/3 of their cohort (mainly from CIS countries) could benefit from the new drugs
- Presenting the WHO recommended basic aDSM as a complex pharmacovigilance slowing down the uptake seems quite exaggerated.
Reviewer #3:
1) Figure 1 - I think it would be stronger if you added graphically to it the estimated number of smear tests - to show the GeneX growth in the context of smear usage
2) Diagnostics section - when you mention private sector I think you are wasting an opportunity - the issue is not just with concessionary pricing it's that there is no effective oversight and no political leadership to assure quality of diagnosis and care in the private sector.
3) Paragraph three - I would calculate the estimated number of patients that need access to these drugs (480K *1/3 = 160K annually) to emphasize how far off the mark we are with 7000 ttt's total. This would strengthen the deficit
https://doi.org/10.7554/eLife.25956.005Author response
Reviewer 1
1) Although there is nothing wrong in publishing this article as such, considering the authors' expertise, vast experience in the field of TB and other infectious diseases, they should also include few constructive suggestions on the above aspects than being generic.
Thank you. We agree and have provide several constructive suggestions towards the end of the revised version. Please see the revised section on Silver linings and potential solutions.
2) Also, often time researchers ignore the necessity to concentrate more on the follow-up of TB cases started on treatment, and bacteriological confirmation at various time points to ensure the completion of treatment and disease free status. There is no diagnostic test available at present to differentiate dead and viable bacteria. Even the famous Bangladesh study relied only on vital staining techniques such as FDA/ EB based microscopy to prove that the MDR cases are not secreting non-viable bacilli. Considering this need, the authors must urge the scientific community to concentrate on this aspect as well.
Our article was about low access to TB innovations that already exist. We agree that a test for cure is necessary, but we would like to avoid listing all the unmet needs in TB, since that is not the goal of our paper.
3) People generally tend to ignore paediatric and extra-pulmonary TB cases due to diagnostic constraints. Although XPert does wonders in the early detection of such cases, access becomes difficult and also specimen collection, which requires additional provision including hospitalization, negates the optimal utility of XPert. With any new technique when the sensitivity gets enhanced, the danger of quality being compromised lingers on. To overcome this, the necessity to establish quality assurance in public and private care should be included.
We have added the following text to address this:
‘Children are an especially vulnerable population when it comes to TB and MDR-TB and although tools like Xpert have been endorsed for use in children (WHO policy), and Xpert has been shown to greatly improve the detection of MDR-TB in children (Raizada et al), access remains a concern in this subgroup.’
4) Likewise, the easy access and availability of drugs in suitable formulations for paediatric TB cases should be advocated. This applies more so for newer drugs.
Children have been virtually overlooked when it comes to access to the new drugs, even though delamanid was recommended by the World Health Organization for children as young as six years of age in 2016 (World Health Organization, 2016). Such exclusion is often a perverse result of a desire to “protect” children from the unknown adverse events of novel agents, a practice that is especially concerning given the well-known toxicity of the injectable agents (Weld, E., et al., 2017). Not only is there a need to include children earlier in the clinical trials of novel agents (Nachman et al., 2015) but also to develop child-friendly formulations of the medications (Furin et al., 2015), something that is being pursued with both bedaquiline and delamanid. Other populations vulnerable to exclusion include pregnant women and persons with extrapulmonary TB, and countries should make plans for off-label use of new drugs in these individuals should the benefits outweigh the risks.
5) The upcoming improved version of Xpert such as XPert Ultra, Omni and other methods such as TB LAMP, True NAT etc may also be mentioned to show that some hope is on the horizon.
We have added a note about the recent WHO endorsement of Xpert Ultra and other newer tools.
6) Finally TB control should be inclusive and we are all aware that involving private care remains mostly on paper now for various reasons. Until the respective governments give their commitment by way of legislation or decree, we will be rendering mostly lip service and any amount of writing may not solve the problem. This may be advocated in the UN Assembly as and when they hold a special session on TB Control. Can this be considered by the authors and also other points submitted.
We have added the following text to the article:
‘There has been almost no involvement of the private sector in the use of new drugs, even in private sector facilities that have a proven track record in the successful management of MDR-TB (Udwadia et al., 2016).’
Reviewer 2
1) The authors omit to mention that Bdq and Dlm are not fully approved by any SRA but got either accelerated or conditional approval by FDA or EMA after their phase IIb. This justifies the pharmacovigilance requirements and partly explains the reluctance of some countries to use these drugs.
We added the term “conditionally approved” to the manuscript.
2) The paper fails to recognize and describe the major obstacles that lie at country level (regulatory authorities, NTPs, or reluctance from clinicians): India which is eligible to GF is limiting access to Bdq to 6 centers of excellence for a country of 1.3 billion inhabitants; Peru, despite registration and free access to Bdq has only enrolled 71 patients, Philippines 51, etc.
Most of the barriers mentioned here are discussed in the text. However, in order to emphasize their importance, we have added the following sentence:
Other important country-level barriers seem to be driving the slow uptake of new drugs on the part of regulatory agencies, NTPs, and clinical providers.
3) Presenting the cost as a major obstacle to access is somehow contradicted (or at least tempered) by the facts: there is very little uptake of Bdq by most GF eligible countries for which Bdq is free (numerous examples: Peru, Kyrgyzstan, Bangladesh, India, etc.) when South Africa (which pays Bdq at 900 USD per treatment because of internal procurement mechanism) is far ahead with over 4,000 treatments.
We thank the reviewer for pointing this out. We have added the following sentence to the paragraph to show that cost is not the only barrier to bedaquiline use.
Some countries, however, have recognized that the cost of purchasing bedaquiline is lower than the health systems costs of ongoing spread of MDR-TB, as seen in the successful South African program. South Africa has to purchase its own bedaquiline yet it accounts for more than 60% of the global use (Ndjeka et al., 2016)
4) There is no doubt that the WHO recommendations on new drugs should be revised, however most countries are far from even reaching the current WHO recommended indications. One could quite easily make estimates showing that following these recommendations "to the letter", as the authors say, would rather result in a much greater uptake than what is actually observed.
We have added the following statement in to address the reviewer’s concerns:
‘It should be noted, however, that most countries are unable to implement new drugs even following these restrictive recommendations.’
5) Minor comments
-77 million sputum smears is a bit misleading as it includes the follow-up smears
We have added a note that this includes follow-up smears.
- Presenting the costs of the new drugs in high income countries is not relevant to the scope of the paper
We disagree with this, as the high costs have greatly limited access to the new drugs in wealthier countries, and they are reserved only for the sickest patients. Pricing is an issue and we feel it is important to mention the range of prices.
- I would suggest referencing the WHO guidelines for Xpert, LPA, LAM, etc.
We have added these references
- Bonnet et al. found that 2/3 of their cohort (mainly from CIS countries) could benefit from the new drugs
We have added the following text to the paper to address the reviewer’s concerns: although some studies suggest that as many as two-thirds of patients would benefit from the new drugs (Bonnet, Bastard et al. 2016)
- Presenting the WHO recommended basic aDSM as a complex pharmacovigilance slowing down the uptake seems quite exaggerated.
While we appreciate the reviewer’s opinion on this topic, data on early barriers to using new drugs was collected as part of the work reported in the Furin et al., 2016 article. A majority of the countries named the need for active PV as a significant barrier to introduction. Most TB programs use passive reporting systems, and in some countries, no PV system existed at all. Because this was reported by countries as a major reason for not introducing the new drugs, we prefer to keep it in the paper, even if the reviewer feels it is an exaggeration.
Reviewer 3
1) Figure 1 - I think it would be stronger if you added graphically to it the estimated number of smear tests - to show the GeneX growth in the context of smear usage
We have a separate paper in preparation, on the Smear to Xpert cartridge ratio across 22 HBCs. Since that work is not published, we are not able to add the estimated smear numbers to the existing Fig 1.
2) Diagnostics section - when you mention private sector I think you are wasting an opportunity - the issue is not just with concessionary pricing it's that there is no effective oversight and no political leadership to assure quality of diagnosis and care in the private sector.
We agree and have noted this in the revised version:
In addition, quality of TB care, especially diagnosis, is a concern in the private sector (Das, Kwan et al. 2015). This requires a comprehensive private sector engagement that includes quality improvement strategies (Cazabon, Alsdurf et al. 2017).
3) Paragraph three - I would calculate the estimated number of patients that need access to these drugs (480K *1/3 = 160K annually) to emphasize how far off the mark we are with 7000 ttt's total. This would strengthen the deficit
DR-TB STAT, the organization whose work is cited here, takes a more conservative approach to estimating new drug needs, and they base it not on the estimated 580,000 persons with RR-TB each year, but rather on the numbers of persons actually started on treatment. In order to address this concern, we have added the following statement:
although some studies suggest that as many as two-thirds of patients would benefit from the new drugs (Bonnet, Bastard et al. 2016)—meaning that there are between than 200,000 and 400,00 persons in need of the novel medications. Even a more conservative estimate based on the number of persons actually started on MDR-TB treatment each year reveals a major access gap among the 41,667 patients who urgent need these medications.
Overall in this section I think you are missing a major part of the narrative. In my opinion, the TB community has collectively failed to get the Phase 3 trials through in a timely manner. It's a little tough to say that the guidelines haven't changed when the pool of data (except observational cohort data) hasn't really moved in 4 years. There are many contributory factors but this is super slow - money, trials sites, regimen design, data access issues yes - but this is another strong signal of the lack of ambition.
We have added the following sentence to the paper to address the reviewer’s concern: Complicating this have been the long delays seen in starting pivotal later stage clinical trials for MDR-TB (RESIST TB, 2017).
https://doi.org/10.7554/eLife.25956.006Article and author information
Author details
Publication history
- Received:
- Accepted:
- Version of Record published:
Copyright
© 2017, Pai et al.
This article is distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use and redistribution provided that the original author and source are credited.
Metrics
-
- 3,292
- views
-
- 400
- downloads
-
- 38
- citations
Views, downloads and citations are aggregated across all versions of this paper published by eLife.
Download links
A two-part list of links to download the article, or parts of the article, in various formats.
Downloads (link to download the article as PDF)
Open citations (links to open the citations from this article in various online reference manager services)
Cite this article (links to download the citations from this article in formats compatible with various reference manager tools)
Point of View: Tuberculosis innovations mean little if they cannot save lives
eLife 6:e25956.
https://doi.org/10.7554/eLife.25956
Further reading
-
- Epidemiology and Global Health
- Microbiology and Infectious Disease
Background:
In many settings, a large fraction of the population has both been vaccinated against and infected by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Hence, quantifying the protection provided by post-infection vaccination has become critical for policy. We aimed to estimate the protective effect against SARS-CoV-2 reinfection of an additional vaccine dose after an initial Omicron variant infection.
Methods:
We report a retrospective, population-based cohort study performed in Shanghai, China, using electronic databases with information on SARS-CoV-2 infections and vaccination history. We compared reinfection incidence by post-infection vaccination status in individuals initially infected during the April–May 2022 Omicron variant surge in Shanghai and who had been vaccinated before that period. Cox models were fit to estimate adjusted hazard ratios (aHRs).
Results:
275,896 individuals were diagnosed with real-time polymerase chain reaction-confirmed SARS-CoV-2 infection in April–May 2022; 199,312/275,896 were included in analyses on the effect of a post-infection vaccine dose. Post-infection vaccination provided protection against reinfection (aHR 0.82; 95% confidence interval 0.79–0.85). For patients who had received one, two, or three vaccine doses before their first infection, hazard ratios for the post-infection vaccination effect were 0.84 (0.76–0.93), 0.87 (0.83–0.90), and 0.96 (0.74–1.23), respectively. Post-infection vaccination within 30 and 90 days before the second Omicron wave provided different degrees of protection (in aHR): 0.51 (0.44–0.58) and 0.67 (0.61–0.74), respectively. Moreover, for all vaccine types, but to different extents, a post-infection dose given to individuals who were fully vaccinated before first infection was protective.
Conclusions:
In previously vaccinated and infected individuals, an additional vaccine dose provided protection against Omicron variant reinfection. These observations will inform future policy decisions on COVID-19 vaccination in China and other countries.
Funding:
This study was funded the Key Discipline Program of Pudong New Area Health System (PWZxk2022-25), the Development and Application of Intelligent Epidemic Surveillance and AI Analysis System (21002411400), the Shanghai Public Health System Construction (GWVI-11.2-XD08), the Shanghai Health Commission Key Disciplines (GWVI-11.1-02), the Shanghai Health Commission Clinical Research Program (20214Y0020), the Shanghai Natural Science Foundation (22ZR1414600), and the Shanghai Young Health Talents Program (2022YQ076).
-
- Epidemiology and Global Health
Background:
The role of circulating metabolites on child development is understudied. We investigated associations between children’s serum metabolome and early childhood development (ECD).
Methods:
Untargeted metabolomics was performed on serum samples of 5004 children aged 6–59 months, a subset of participants from the Brazilian National Survey on Child Nutrition (ENANI-2019). ECD was assessed using the Survey of Well-being of Young Children’s milestones questionnaire. The graded response model was used to estimate developmental age. Developmental quotient (DQ) was calculated as the developmental age divided by chronological age. Partial least square regression selected metabolites with a variable importance projection ≥1. The interaction between significant metabolites and the child’s age was tested.
Results:
Twenty-eight top-ranked metabolites were included in linear regression models adjusted for the child’s nutritional status, diet quality, and infant age. Cresol sulfate (β=–0.07; adjusted-p <0.001), hippuric acid (β=–0.06; adjusted-p <0.001), phenylacetylglutamine (β=–0.06; adjusted-p <0.001), and trimethylamine-N-oxide (β=–0.05; adjusted-p=0.002) showed inverse associations with DQ. We observed opposite directions in the association of DQ for creatinine (for children aged –1 SD: β=–0.05; pP=0.01;+1 SD: β=0.05; p=0.02) and methylhistidine (–1 SD: β = - 0.04; p=0.04;+1 SD: β=0.04; p=0.03).
Conclusions:
Serum biomarkers, including dietary and microbial-derived metabolites involved in the gut-brain axis, may potentially be used to track children at risk for developmental delays.
Funding:
Supported by the Brazilian Ministry of Health and the Brazilian National Research Council.




{kind=link}
{kind=link}